
1) Welcome to @cardiomet_CE's new series on #lipid management! This is a 10-#tweetorial program, all #accredited, that will cover it all. Our first expert author is Paul Thompson MD @PaulDThompsonMD, esteemed #cardiologist from @hartfordhosp @UConn Med & now @MGHHeartHealth !
2) This #tweetorial, accredited for #CME/CE and intended for #physicians #physicianassociates #nurses #nursepractitioners #pharmacists is supported by an educational grant from Esperion Therapeutics. See faculty disclosures at https://cardiometabolic-ce.com/disclosures/.
3) @PaulDThompsonMD took on education re mechanisms & use of ezetimibe & bempedoic acid. He proposes a case: 45 ♂️ w/history of inferior wall #MI treated with primary angioplasty.
4) He is referred because he refuses to take statins because they produce what he calls, “intolerable muscle aching”. He has tried atorvastatin, rosuvastatin, and pravastatin in standard doses, and he developed discomfort with each of these medications. What would you do?
5) It is always appropriate to encourage such patients to retry the #statin since statins are life-saving drugs, but it is also important not to push the statins so hard that you alienate the patient and because there are other available options.
6) This man has failed standard doses of statins, & may refuse additional statin trials, but one approach is to try extremely low doses of a long-acting statin. Long-acting statins include #atorvastatin, #rosuvastatin, and #pitavastatin.
7) These statins can be given thrice twice or even twice weekly, and still produce impressive reductions in low-density lipoprotein cholesterol (#LDL-C).
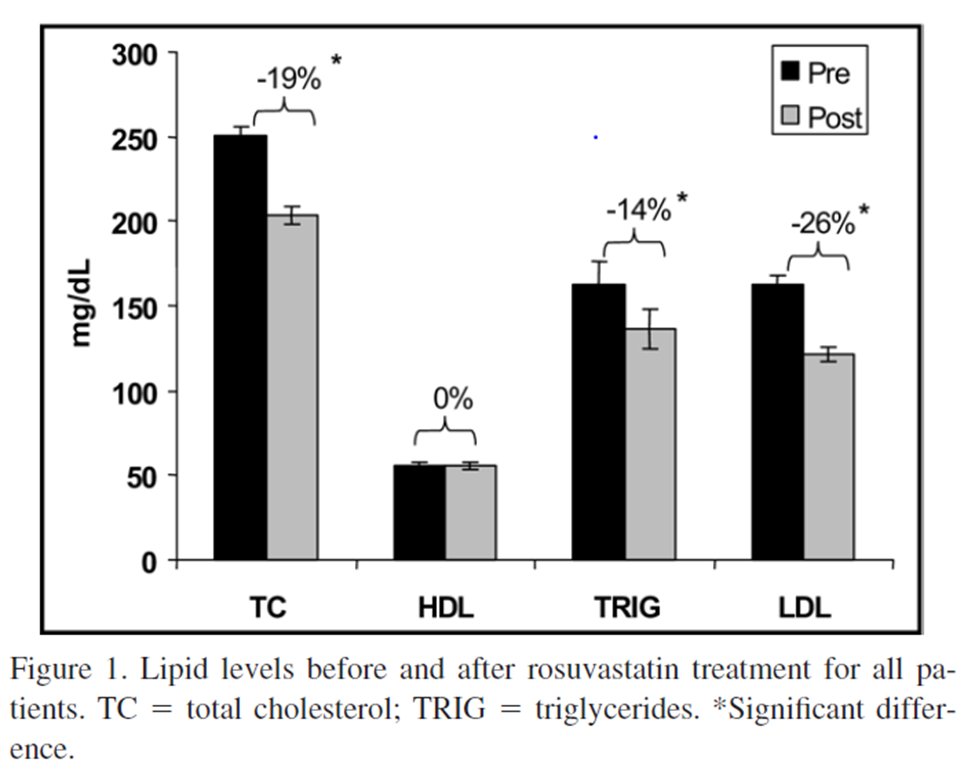
8) We prescribed rosuvastatin 5 (n=30) or 10 (n=10) mg twice weekly to 40 of my patients complaining of statin associated muscle symptoms (#SAMS). We measured lipids ≥ 3 weeks after starting treatment & on the morning before their next statin dose.
9) LDL decreased 26% despite the very low doses. Most patients (n=32) tolerated the low-dose statin over a mean follow-up of 3 months (range 2 – 12 mos), but 8 could not.
10) This low-dose statin approach is off-label & most cholesterol management guidelines recommend moderate or high-dose statins. Guidelines are based, whenever possible, on randomized clinical trial (#RCT) data and few RCTs have used low dose statin therapy.
11) High dose-statin therapy is superior to low doses in reducing cardiac events (CTTC at 🔓 https://pubmed.ncbi.nlm.nih.gov/21067804/), but some LDL reduction is probably better than none & low-dose statins produce fewer side effects.
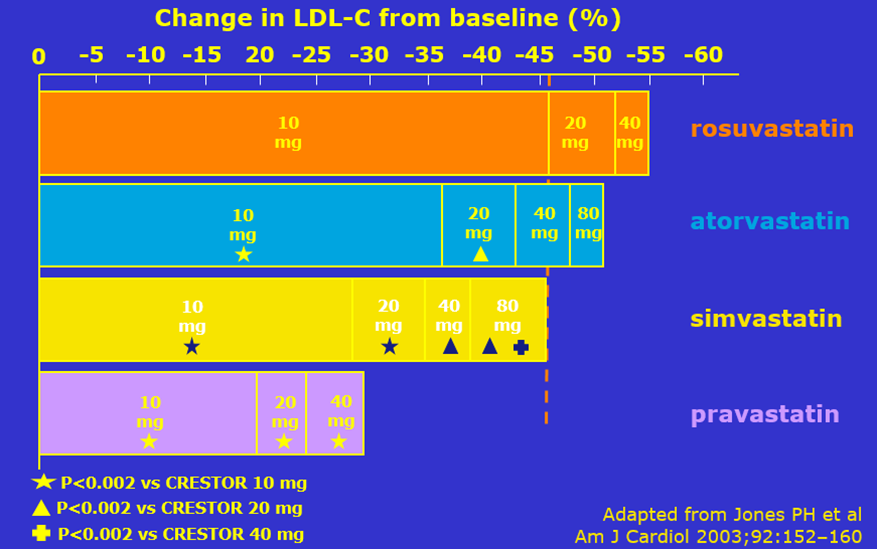
12) Statins do produce the greatest⬇️LDL-C with the highest statin dose, but greater⬇️LDL-C per mg of drug happens w/low doses. This is the “Statin Rule of 6”, which refers to the observation that each doubling of a statin dose produces only 6% of the baseline additional LDL-C⬇️.
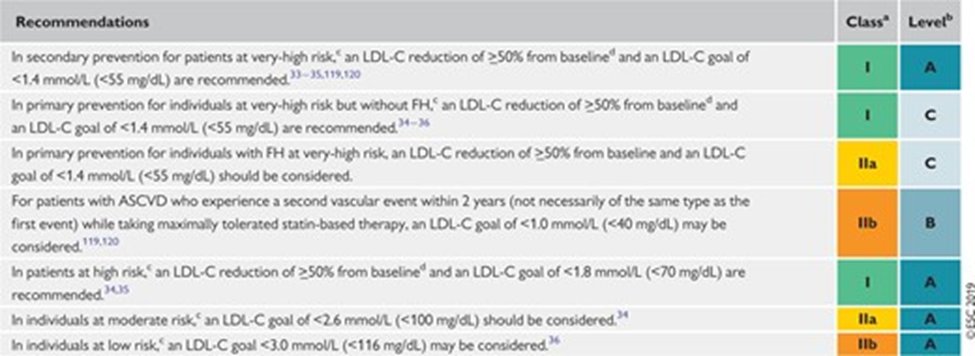
13) Let’s say that our 45y/o #MI survivor had an untreated LDL-C of 200 mg/dL. That is too high for a pt with #CAD; the most recent 2018 cholesterol management guidelines recommend LDL cholesterol < 70 mg/dL for such patients (shown below, from 🔓https://pubmed.ncbi.nlm.nih.gov/30423391/).
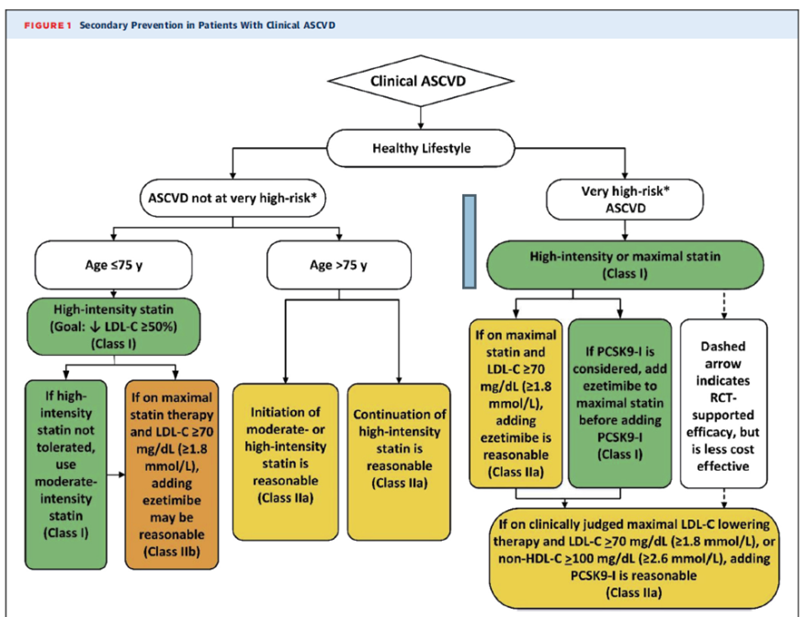
14) Our European colleagues are even more aggressive and recommend an LDL <55 mg/dL for such patients. See 🔓https://academic.oup.com/eurheartj/article/41/1/111/5556353).
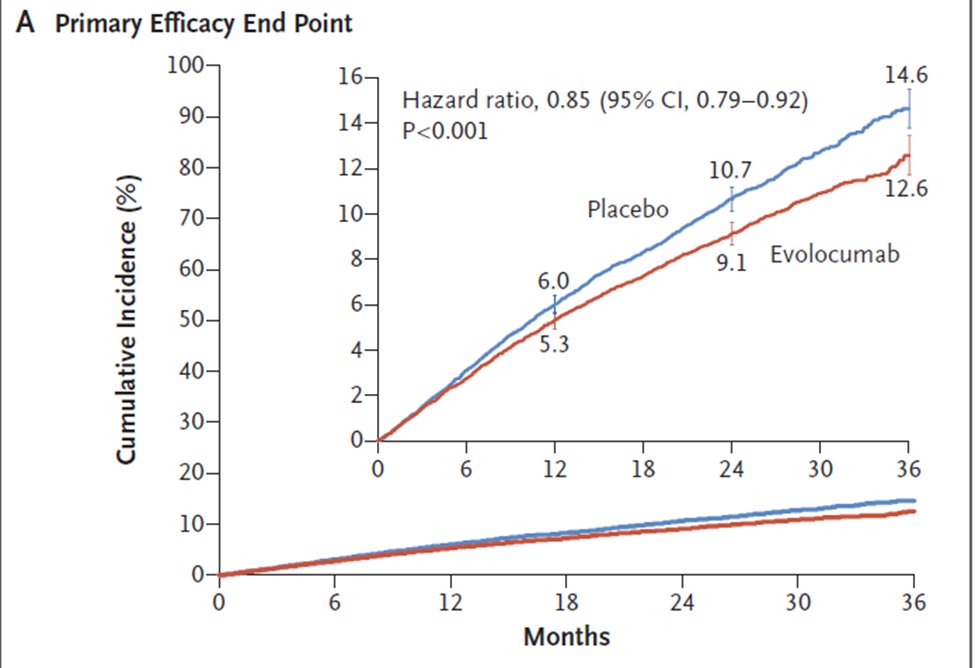
15) Indeed, with respect to reducing subsequent events in patients with known CAD, the rule is that “even lower is even better”. The best proof of this is the FOURIER trial (🔓https://www.nejm.org/doi/full/10.1056/NEJMoa1615664). All 27,564 subjects in FOURIER had #ASCVD and were considered …
16) … high risk for reoccurrence. They had baseline LDL-C levels ≥ 70 mg/dl, the current goal for CAD patients. Subjects were randomized to the proprotein convertase subtilisin–kexin type 9 inhibitor (#PCSK9i) evolocumab or to placebo.
17) On treatment median LDL-C levels were 30 mg/dl in the PCSK9i group & ~90 mg/dl in the placebo group. Over 3y follow-up, there was 2% absolute⬇️in the combo of CV death, myocardial infarction, stroke, hospitalization for unstable angina, & coronary revascularization.
18) So because “even lower is even better" we should use all our weapons, including #ezetimibe & #bempedoic acid alone or in combination, to lower LDL-C levels if the first line drugs–#statins–do not produce sufficient LDL ⬇️or are not tolerated.
19) Returning to our 45-year-old with an LDL-C of 200, if we start him on pravastatin 20 mg daily, his LDL-C will ⬇️approximately 25%, or ~50 mg/dL. His LDL should go from 200 to 150 mg/dl, still nowhere near our < 70 mg/dL goal.
20) When we double the dose, tho, we don't get another 25%⬇️of the baseline LDL-C value; remember the rule from Tweet 12? We get only an additional 6% ⬇️=12 mg/dL. This leaves him with an LDL-C of 138, plus he has had statin intolerance so is probably not a fan of ANY 2x dose!
21) The news is even worse for high doses of the most powerful statins. Going from 20 mg daily of rosuvastatin to 40mg or from 40 mg of atorvastatin to 80, produces only an additional 3-4% LDL-C reduction.
22a) So the take-home messages so far: (a) statins are life-saving medicines & we should do our best to encourage patients to use them (b) statins produce large LDL⬇️with very little drug, w/higher statin doses produce diminishing LDL–C reductions.
22c) And some ⬇️ is better than none, esp since we can add on other agents, like #ezetimibe & #bempedoicacid. So here's a knowledge check: how does ezetimibe work?
— cardio-met (@cardiomet_CE) March 22, 2022
a) reduces GI cholesterol absorption
b) breaks down cholesterol in the liver
c) prevents LDL-C synthesis
23) Mark your answer and return tomorrow for more expert-led education on #lipid management! Hello to @JJheart_doc @NMHheartdoc @harvardmed @Drlipid @GoggleDocs @ProfKausikRay @PamTaubMD @cpcannon @lipiddoc @CBallantyneMD @ErinMichos @DrMarthaGulati @rgiugliano @MarcBonaca
24) Welcome back! You're learning about re mechanisms & use of ezetimibe & bempedoic acid from @PaulDThompsonMD, while you earn 0.5h CE/#CME! This is part of a unique #tweetorial series here on @cardiomet_CE. And a tip o' the hat to @DrMichaelShapir @DoctorLatina @rblument1
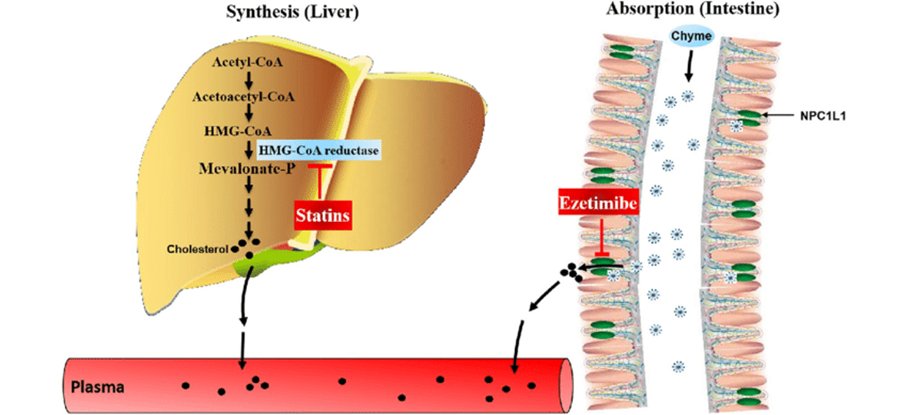
25) So, about #ezetimibe. It inhibits the absorption of cholesterol from the gut. Some patients (& clinicians) worry that ezetimibe will not work on patients with low dietary cholesterol intakes, but most of the cholesterol in the gut comes from biliary cholesterol.
26) Therefore ezetimibe works very well in even the most dietary conscientious patients. By interfering with intestinal #cholesterol absorption, less cholesterol comes to the liver via the portal circulation. This decreases hepatocyte cholesterol content and …
27) … prompts the liver to make more LDL-C receptors, which do the hard work of reducing blood cholesterol. Ezetimibe produces about a 20%⬇️in LDL-C cholesterol when used alone and a slightly larger reduction, about 24%, when added to a #statin.
28) The fact that ezetimibe works by⬆️LDL receptor activity is important because all drugs & other strategies that ⬆️LDL receptor activity are assoc'd w/⬇️#ASCVD clinical events. A meta-analysis of lipid-lowering therapies demonstrated that the⬇️in #ASCVD events is …
29) … similar among multiple meds & other strategies when adjusted for magnitude of LDL-C reduction ( 🔓https://jamanetwork.com/journals/jama/fullarticle/2556125). So to repurpose two common phrases, “It’s the LDL, Stupid”, and with respect to LDL-C, “Just re-duce it”.
30) Many clinicians question ezetimibe’s clinical effectiveness. I have called ezetimibe “the Rodney Dangerfield of lipid-lowering agents” because just like poor Rodney, it gets no respect. Questions about its effectiveness arose from a flawed study called ENHANCE.
31) ENHANCE (🔓https://www.nejm.org/doi/full/10.1056/nejmoa0800742) randomized patients with familial hypercholesterolemia to simvastatin 80 mg w/ or w/o ezetimibe 10 mg daily. The average LDL-C cholesterol off any lipid-lowering medications was 318±66 mg/dL, but subjects were recruited …
32) … from excellent lipid clinics and their LDL-C had been well-treated prior to their enrollment. LDL-C was reduced to 193±60 with simvastatin and to 141±53 mg/dL with simvastatin plus ezetimibe. The primary outcome was change in carotid intima-media thickness (IMT) but …
33) … carotid IMT was normal at baseline in both groups probably because they had been so well-treated. Now here’s a big surprise. CMT was still normal after 2y of the study; there was no difference between the 2 groups.
34) Obviously, it is hard to make something that is normal more normal, but this study was interpreted publicly by multiple national “experts” as showing ezetimibe was a “placebo”. This skepticism about ezetimibe’s effectiveness still exists albeit to a much lesser extent.
35) Even a subsequent #RCT showing that ezetimibe improved cardiac outcomes did not totally fix ezetimibe’s damaged reputation. IMPROVE-IT (🔓https://www.nejm.org/doi/full/10.1056/nejmoa1410489) randomized pts w/ #ACS to simvastatin 40 w/ or w/o ezetimibe.
36) Combination statin+ezetimibe➡️2% absolute⬇️ASCVD events 34.7⤵️32.7% (p= 0.016), but the study was widely criticized because it had to be extended because there were so few events in both groups. Consequently, results were reported after a median of 6 years follow-up …
37) … a long time for most #RCTs of lipid-lowering therapy. I think it took so long to see an effect because the on-treatment LDL cholesterols were low in both groups & only slightly lower in the ezetimibe group at (53.7 vs 69.6). Remember, ⬇️LDL-C values⬇️ ASCVD events.
38) Interestingly, the absolute⬇️w/ezetimibe in CV events was 0.9% for pts <age 65, 0.8% for age 65-75, but a whopping 8.7% in those ≥65. Among patients ≥ 75 only 11 needed to be treated to prevent 1 event. Among patients < 75, 25 needed to be treated to prevent one event.
39) The riskiest group in any study gets the best absolute risk⬇️, & age is a powerful ASCVD risk factor, but this magnitude of “age discrimination” is not as pronounced to my knowledge with other lipid-lowering interventions.
40) It is not apparently due to differences in cholesterol absorption with age, because the lipid response to ezetimibe did not differ among the 3 age groups. We could treat the 46♂️ who does not want to take a statin with ezetimibe alone or if he were willing, with ezetimibe …
41) … plus a low-dose statin. But if he totally refuses a statin another possible choice is bempedoic acid w/ or w/o ezetimibe. How does bempedoic acid work?
a) inhibits HMG-CoA reductase
b) inhibits ACLY
c) prevents GI absorption of lipids
d) increases # LDL-C receptors
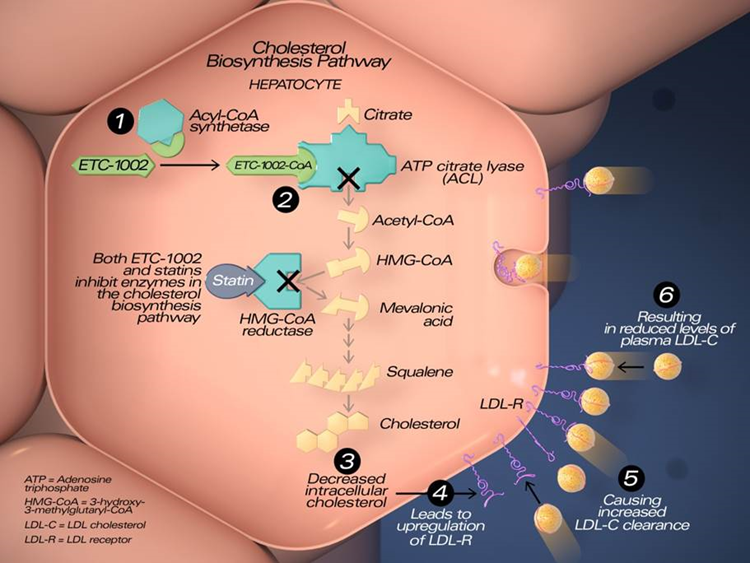
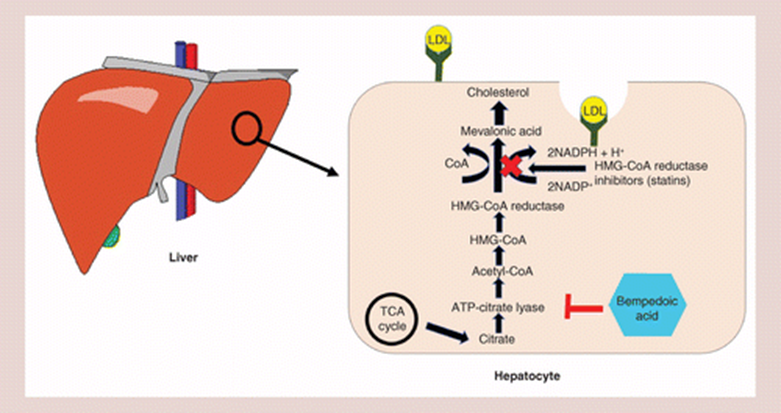
42) Statins inhibit hydroxymethylglutaryl-CoA (HMG-CoA) reductase, the rate-limiting enzyme in the mevalonate cholesterol synthesis pathway. They ⬇️hepatic cholesterol production thereby ⬇️intrahepatocyte cholesterol➡️⬆️production of LDL-C receptors, which …
43) … extract LDL-C from the blood & ⬇️blood LDL-C. #Bempedoic acid, formally(ETC-1002), is not a statin, but works in the same mevalonate-cholesterol production pathway as statins, where it inhibits ATP-citrate lyase (ACLY), an enzyme upstream from HMG-CoA reductase.
44) Bempedoic acid was developed because it may have fewer, if any, muscle side-effects. It is administered orally as a pro-drug that must be activated by being converted into its active form bempedoyl-CoA by very long-chain acyl-CoA synthetase (🔓https://pubmed.ncbi.nlm.nih.gov/35031766/Batchuluun).
45) This enzyme is abundant in the liver, but not in skeletal muscle. Consequently any un-acetylated bempedoic acid that escapes the liver and first pass hepatic metabolism should not be able to affect skeletal muscle where it cannot be activated.
46) The reduction in LDL-C with bempedoic acid is quite robust, but not as strong as statins. I @PaulDThompsonMD reported its first use in statin-intolerant subjects; they achieved a 33%⬇️in LDL-C (28.7% > placebo) with bempedoic acid 180mg/dl, the recommended dose.
47) This is greater than the 17-18% reduction predicted in the drug’s package insert, but some of the patients in the studies generating the 18% data were also on “maximally tolerated statins”. None of the subjects in my study used concomitant statins.
48) Bempedoic acid is also available w/ezetimibe as a combo therapy. The PI suggests that the combo can ⬇️LDL-C by 38%, based on a study in which only 35% of subjects were not on a statin (🔓https://pubmed.ncbi.nlm.nih.gov/31357887/).
49) This study did not examine if there was a difference in response between statin-treated & not-statin treated subjects when given the combination agent.
50) Clinicians should be aware of 2 side effects of bempedoic acid; it can⬆️uric acid levels by interfering with uric acid excretion into the renal tubule. I usually check UA levels in pts before starting drug & think twice about using bempedoic acid in pts w/a history of gout.
51) Bempedoic acid can also⬆️creatinine, again by interfering with renal tubule excretion. The #GFR itself is not actually altered but it appears altered when calculated using the higher creatinine.
52) This increase in creatinine is similar to that produced by fenofibrate, which increases creatinine and then returns to baseline when the medication is stopped.
53) Ezetimibe should be considered in pts who do not tolerate statins or who do not achieve their LDL-C goals with statins alone. Similarly, bempedoic acid alone or in combination should also be considered in patients who cannot tolerate statins. Bempedoic acid has not …
54) … been documented to reduce ASCVD events, but studies examining this are ongoing and are likely to demonstrate event reduction because all strategies that increase LDL receptor activity have been associated with reduced ASCVD events (🔓https://pubmed.ncbi.nlm.nih.gov/27673306/).
55) And there you have it! You have just earned 0.5h CE/#CME, so go claim it at http://www.cardiometabolic-ce.com/lipids3 ! I am @PaulDThompsonMD and I invite you to follow @cardiomet_CE for more expert-led education on #lipid management and reduction of #ASCVD risk!

Originally tweeted by cardio-met (@cardiomet_CE) on March 22, 2022.