
Join here tomorrow for the launch of a new #accredited #tweetorial on the mechanism of action of #lipid-lowering drugs. Earn 0.5 CE/#CME credits: #physicians #physicianassistant #nurses #NP #pharmacists! Expert faculty @PamTaubMD
#CardioTwitter #medtwitter @academiccme
1) Welcome to an #accredited #tweetorial on the mechanisms of action of lipid lowering drugs. My focus is #statins, #PCSK9 agents, & #inclisiran. Accredited for 0.50h CE/#CME. I am Pam Taub MD @PamTaubMD, Professor of Medicine at @UCSDHealth.
#FOAMed @MedTweetorials
2) This activity is intended for #healthcare providers & is supported by an educational grant from Esperion. Faculty disclosures at https://cardiometabolic-ce.com/disclosures/.
Prior programs are available for credit on #lipid lowering & other #cardiometabolic topics at
3) #Statins are an “iconic” drug class and have been around for more than 30 years. They are the cornerstone of lipid management, although some patients do have side effects with statins and cannot take them #statinintolerance and need other options for lipid lowering.
4) Which of the following is the mechanism of action of statins?
a) Decrease synthesis of PCSK9 protein
b) Inhibition of HMG-CoA Reductase
c) Inhibition of ATP Citrate Lyase
d) Inhibition of cholesterol absorption from the diet
Mark your answer before you scroll ⬇️!
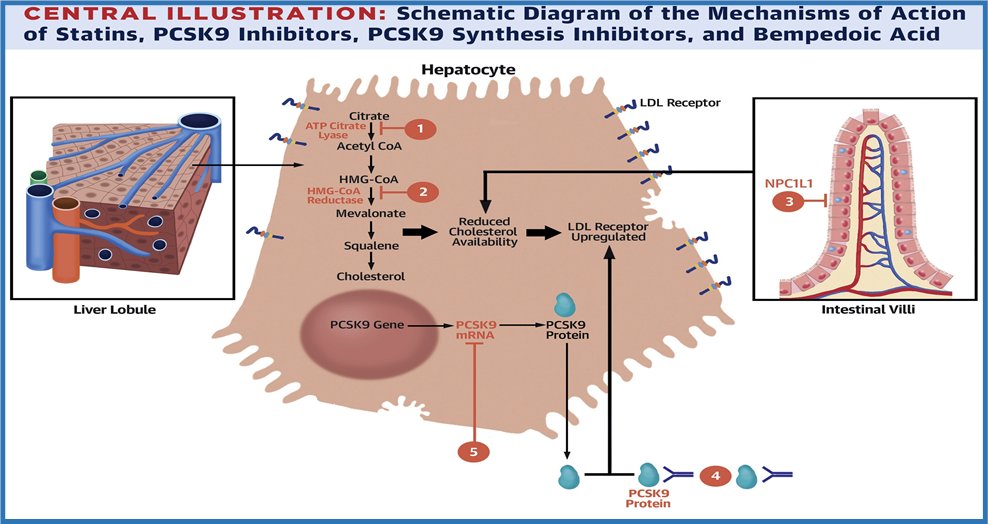
5) The answer is B. Our friend the statin works on the enzyme HMG-CoA Reductase, ⬇️synthesis of #cholesterol in the liver. By ⬇️hepatic cholesterol synthesis, an upregulation of LDL-receptors &⬆️ hepatic uptake of LDL-C from the circulation occurs.
See 🔓
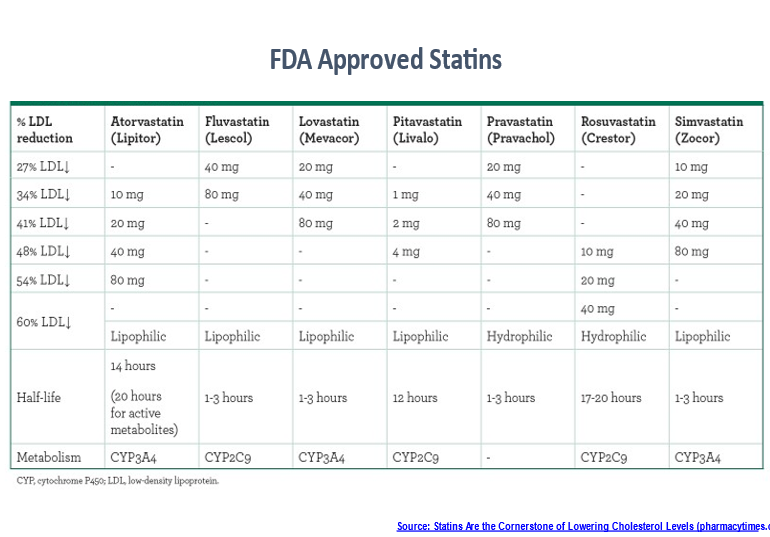
6) The extent of #LDL lowering depends on which statin is used and the dose given.
🔓
7) When statins were first developed, there was uncertainty about whether LDL cholesterol lowering was the right target in reducing #ASCVD risk. There were also concerns about safety, esp cancer risk & nonCV mortality (https://www.nature.com/articles/nrd1112).
8) Over time, large #RCTs such as 4S (https://pubmed.ncbi.nlm.nih.gov/7968073/), WOSCOPS (🔓https://pubmed.ncbi.nlm.nih.gov/7566020/) & HPS (https://pubmed.ncbi.nlm.nih.gov/12114036/) clarified both efficacy re #CV morbidity & mortality in patients and was safe in both primary and secondary ASCVD event protection.
9) In addition to⬇️LDL-C & CV events, statins may have additional pleotropic non–lipid-related effects, inc improvements in endothelial function, stabilization of atherosclerotic plaques, anti-inflammatory, immunomodulatory, antithrombotic effects, effects on bone metabolism . .

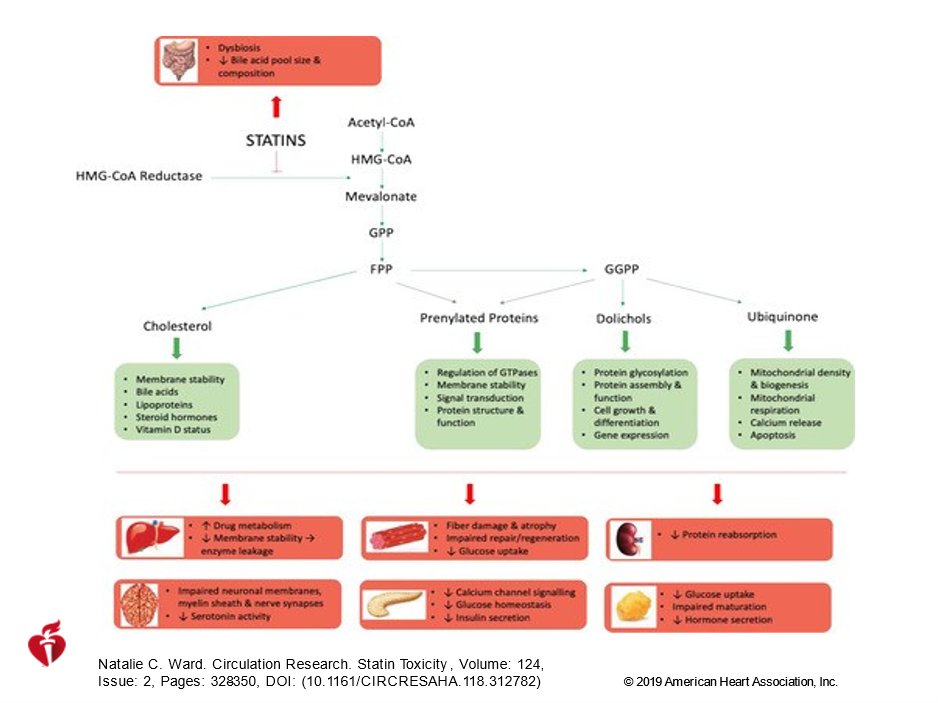
10) … & even reduced risk of dementia. These effects likely arise from statins' inhibition of synthesis of isoprenoid intermediates of the mevalonate pathway. (🔓https://www.ahajournals.org/doi/full/10.1161/CIRCRESAHA.118.312782) and just give us more reasons to use them!
11) That same primary #mechanismofaction–⬇️HMG-CoA Reductase–is also the Achilles' heel for statins; there are also statin receptors in skeletal muscle. The major reason for discontinuation of therapy is statin-associated muscle symptoms (#SAMSs; 🔓https://pubmed.ncbi.nlm.nih.gov/29363784/).
12) #SAMs can present as myalgia, myopathy, myositis with⬆️CPK, or even #rhabdomyolysis. There are also reports of statin-related joint and abdominal pain, tendinopathies & tendon disorders, and arthralgias.
13) Non-SAMs side effects include new-onset T2D, neurological &neurocognitive effects, hepatotoxicity, & renal toxicity. Most of these also relate to the known mechanisms of action (see figure). Nonetheless, for most pts, the efficacy activity predominates.
14) In another tweetorial, @DrMarthaGulati will delve more deeply into statin intolerance. For now & for purposes of this discussion, suffice it to say that there is overwhelming evidence to support lowering LDL-C to⬇️#CV morbidity & mortality, & for most pts, statins do that!
15) Unfortunately, compliance with statins is often not great, even tho we know long-term persistence with statin therapy is important for #CV benefits (https://pubmed.ncbi.nlm.nih.gov/19108805/). Maybe a bigger problem is that in many patients, statin therapy isn't enough to⬇️LDL-C to target.
16) This may occur not only because of "hidden" noncompliance due to SAMs, but importantly from very high baseline levels of LDL-C, as seen in patients with familial hypercholesterolemia (#FH), for whom maximal statin therapy is inadequate even when well-tolerated.
17) This creates a new treatment options or combination therapies that will ultimately translate into improved #CV outcomes. #Ezetimibe was the first non-statin agent introduced on the market. This was followed by the #PCSK9 inhibitors, #bempedoic acid & #inclisiran.
18) Our @cardiomet_CE faculty will➗& conquer here. I'll continue with #PCSK9 inhibitors & #inclisiran, and @PaulDThompsonMD will cover #ezetimibe & #bempedoic acid. But just to be clear, which of the following drugs can you add to statin therapy for further LDL reduction?
19) Mark your best answer and return tomorrow for the answer and more education! @mmamas1973 @pnatarajanmd @DLBHATTMD @RonBlankstein @a_l_bailey @DrHeatherJohn @DBelardoMD @AnnMarieNavar @Drroxmehran @AnastasiaSMihai @DaveDixonPharmD #cardiotwitter @CardioNerds
20) Welcome back to our accredited tweetorial on #lipidmanagment! health! I am @PamTaubMD -let's eradicate the vascular malignancy of #ASCVD! @RpratleyMD @cpcannon @yhandelsmanmd @TYWangMD @CynthiaTaub @amitvkhera @kaulcsmc @drtaranarula @DrRyanPDaly
21) As to our poll from yesterday, the answer is d. #Ezetimibe, #PCSK9 inhibitors, #bempedoic acid & #inclisiran can be ➕to statin therapy. Just as we do with other diseases such as #hypertension we need to be comfortable with combination therapy for managing LDL cholesterol.
22) After ezetimibe, the next class of non-statins approved by the @US_FDA are the #PCSK9 inhibitors.
They are monoclonal antibodies that get rid of the “evil” PCSK9 protein that prematurely degrade the LDL receptor.
23) When it is not “attacked” by PCSK9 protein the LDL receptor is responsible for getting rid of LDL cholesterol from the blood.
🔓
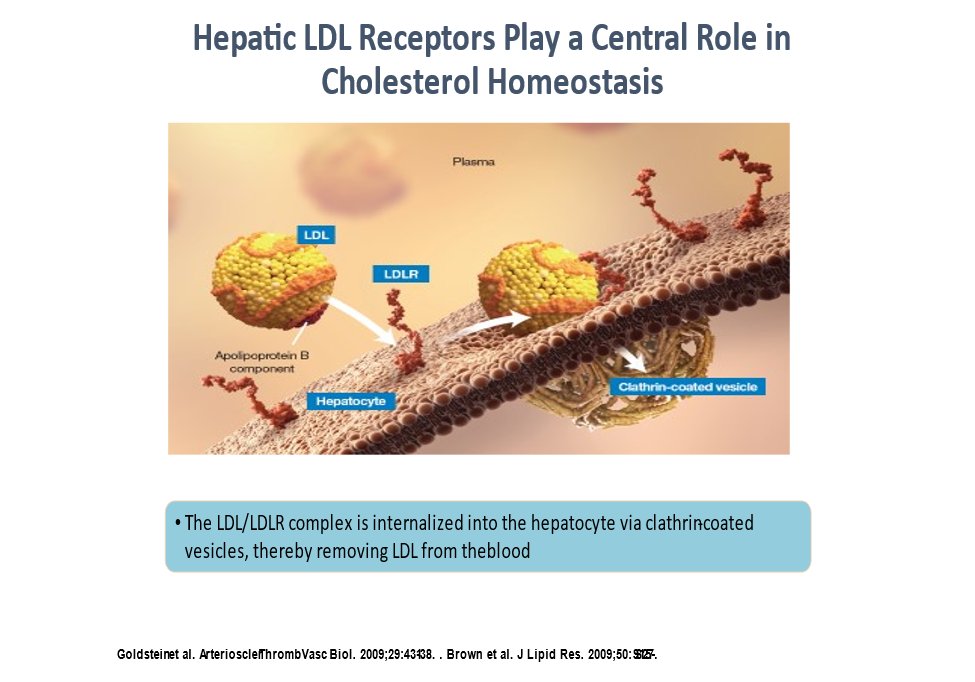
24) It is important that LDL receptor is recycled and not prematurely degraded so that efficient clearance of LDL cholesterol is assured
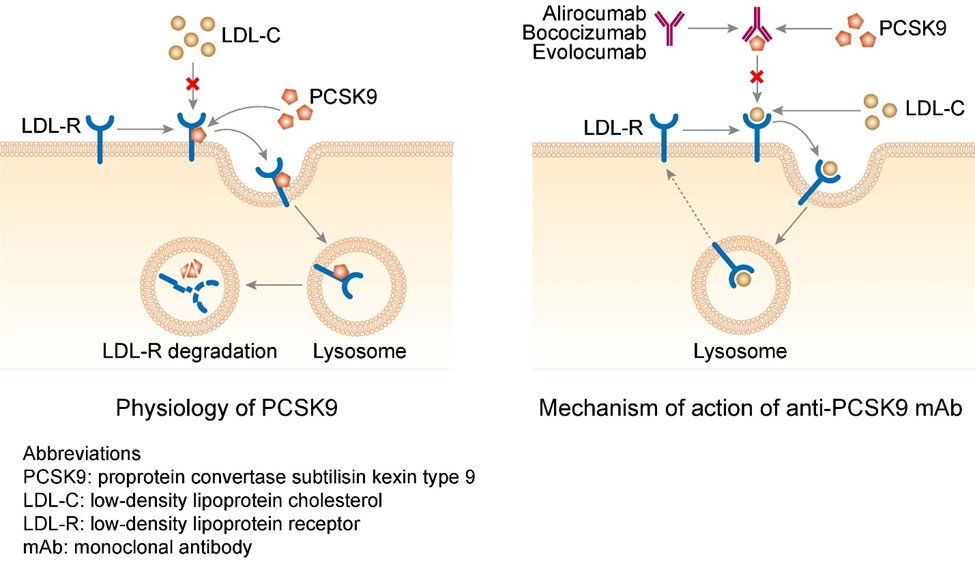
25) Individuals with loss-of-function mutations in PCSK9 have reduced levels of LDL-C and are protected from #CVD (https://www.nature.com/articles/ng1509). Ordinarily, LDL-C binds to LDLRs on the cell surface of hepatocytes, after which PCSK9 binds to LDLR on the hepatocyte surface.
26) Bound PCSK9 then directs the resulting endocytic vesicle to the lysosome for degradation. Lysosomal degradation of the LDLR decreases the concentration of receptors, which are responsible for clearing LDL-C from the bloodstream.
27) When #PCSK9 binding is inhibited, however, LDLRs avoid lysosomal degradation & are recycled to the cell surface to bind more LDL-C particles (🔓https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5079795/). This recycling of LDLRs, due to⬇️bound PCSK9, ➡️⬆️clearance of LDL-C from plasma, thus ⬇️ LDL-C levels.
28) An efficient way to inhibit PCSK9 binding is to use monoclonal antibodies (#mAbs) that target PCSK9; #alirocumab and #evolocumab bind to free PCSK9 in the plasma ➡️ preventing PCSK9 binding to LDLRs (🔓https://www.pnas.org/content/106/24/9820; 🔓https://www.nejm.org/doi/full/10.1056/NEJMoa1105803).
29) The ODYSSEY OUTCOMES (🔓https://www.nejm.org/doi/full/10.1056/nejmoa1801174) & FOURIER (🔓https://www.nejm.org/doi/full/10.1056/nejmoa1615664) trials showed #PCSK9 inhibitors improve #cardiovascular outcomes.
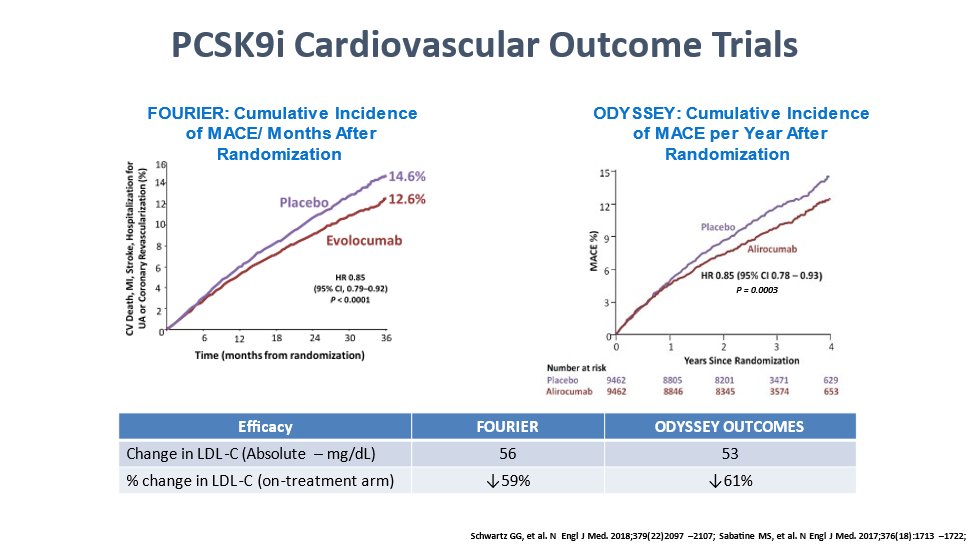
30) With PCSK9 mAbs, a⬇️in LDL-C in a dose-dependent manner, by as much as 70%, (60% in patients on statins) can be achieved. In addition ⬇️ #Lp(a) by 18-36%, ⬇️#triglyceride levels by 12-31%, & ⬆️ HDL-C by 5-9% may be seen.
31) Is there a downside? The available PCSK9 inhibitors appear to be well tolerated and serious AEs are uncommon–similar to placebo. There may be mild injection site reactions (6-10%) and influenza‐like illness or nasopharyngitis.
32) The newest agent is #inclisiran which acts upstream to where PCSK9 inhibitors work. Inclisiran works at the level of the messenger RNA and prevents synthesis of that diabolical PCSK9 protein. It can be given by injection twice a year!
33) So let's get this #mechanismofaction stuff straight. Inclisiran ALSO impacts the PCSK9 enzyme, but unlike PCSK9 inhibitors, which inhibit circulating PCSK9, inclisiran is a bioengineered small interfering RNA (#siRNA) molecule that⬇️production of PCSK9 via gene silencing.
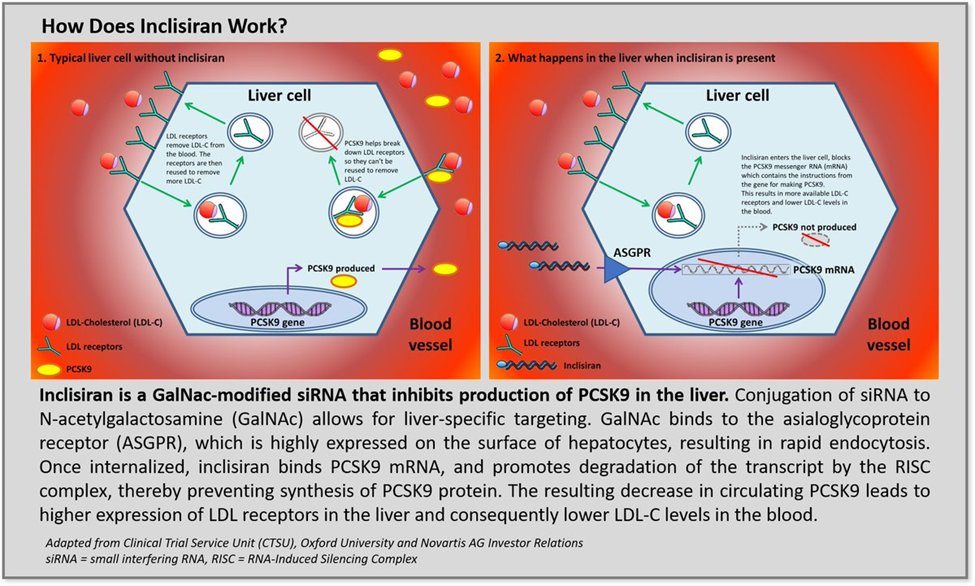
34) Maybe more detail than u want, but it consists of 2 nucleotide strands conjugated to the ligand, triantennary N-acetylgalactosamine (#GaINAc). The ligand targets the drug to the liver by binding specifically to the asialoglycoprotein receptors, which are found . . .
35) … pretty much only on hepatocytes. After binding, inclisiran is taken in by the cell and binds to the RNA-induced silencing complex (#RISC) & the #mRNA encoding PCSK9. The siRNA-RISC complex ✂️the PCSK9 mRNA,🚫synthesis of PCSK9 protein. Even more cool:
36) One siRNA-RISC complex can✂️multiple PCSK9 mRNA. Without PCSK9 enzymes, there will be no lysosomal degradation of the LDL receptor, so LDL-C will bind the receptor, be recycled♻️in the hepatocyte ➡️⬇️ serum LDL-C level.
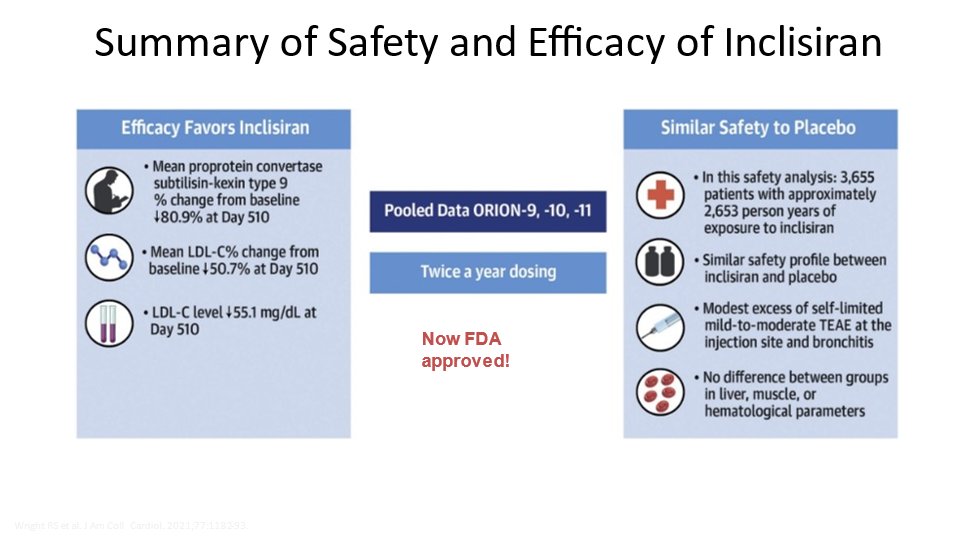
37) Ph 3 pivotal trials (ORION-9, -10, & -11) have demonstrated inclisiran’s significant LDL-C-⬇️effects in patient populations with very high #CV risk, including patients with #FH. It has the potential to be used for both the primary & secondary prevention of ASCVD.
38) The main benefit of inclisiran compared w/PCSK9 mAbs, is the less frequent dosing. About 50% ⬇️in LDL-C levels has been shown in #RCTs with inclisiran. The primary side-effect is again injection site reactions, which tend to be mild.
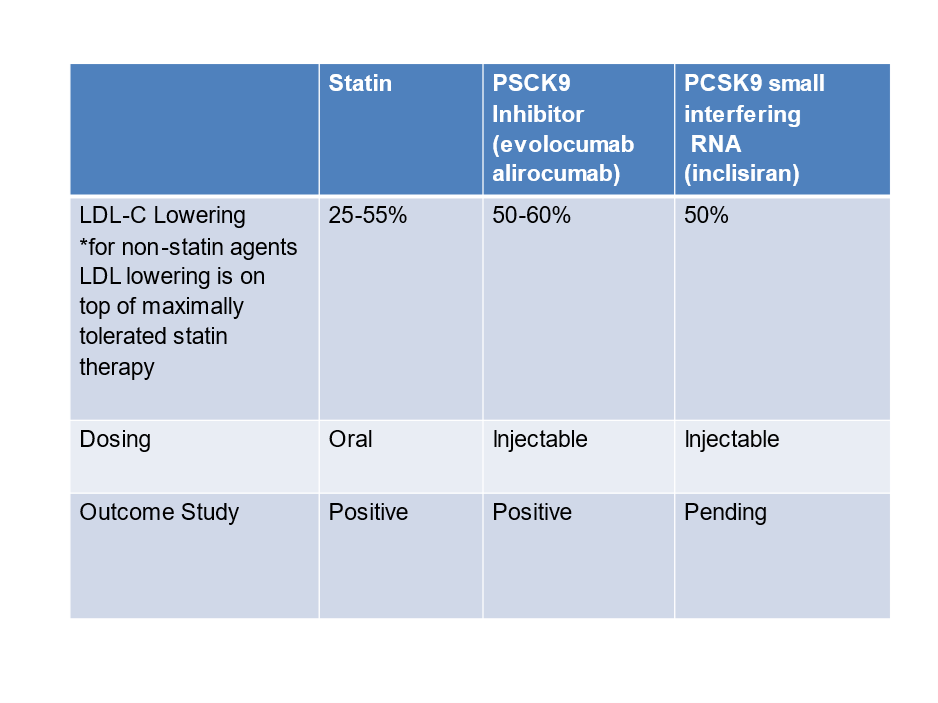
39) Here's a down-n-dirty summary of the agents we have discussed in this #tweetorial:
40) So let's see what you've learned. Which of the following has the most potent LDL lowering effect?
a) rosuvastatin
b) pravastatin
c) evolocumab
d) inclisiran
Mark your answer before you scroll down. And BTW, Where else can you learn on Twitter AND earn CE/#CME??
41) No suspense: The answer is C. The #PCSK9 inhibitor evolocumab gives you the most potent LDL reduction at 50-60%. Statins, though, are the cornerstone of therapy in patients with hyperlipidemia. Ezetimibe & PCSK9 inhibitors⬇️LDL-C & improve #CV outcomes.
42) Bempedoic acid and inclisiran are promising new agents for LDL lowering & outcomes studies are pending. Again, you'll learn ALL about ezetimibe & bempedoic acid from my learned colleague @PaulDThompsonMD in a separate tweetorial here on @cardiomet_CE.
43) You can use these agents together! For my very high risk pts, I have used maximally tolerated statin, ezetimibe, bempedoic acid & PCSK9 inhibitor. Don't be shy about using combo therapy in the mgt of hyperlipidemia. Nods to
@ProfKausikRay @VietHeartPA @fikkumamoto @iamritu
44) And that's it! Go GRAB your CE/#CME certificate for 0.5h credit at http://www.cardiometabolic-ce.com/lipids2 and FOLLOW us here for more🆓education from expert authors in #lipidmanagement & #cardiometabolic medicine. I am @PamTaubMD, shouting out also to
@DrRachelMBond @NehalMehtaMD #FOAMed
Originally tweeted by cardio-met (@cardiomet_CE) on February 22, 2022.